Multiple hereditary exostoses (MHE) is a genetic condition in which a patient has many bone/ cartilage tumors. It is also know as
multiple hereditary osteochondromatosis. These are "tumors"- unregulated growths- but these are not malignant tumors (since they don't go anywhere- they don't metastasize). This condition differs from a condition I have previously posted: isolated
osteochondroma. The tumor is the same (
osteochondroma) but these conditions differ based on how many osteochondromas exist. In
multiple hereditary exostoses, there can be any number of tumors and they can be located just about anywhere in the body: long bones, short bones, scapula, ribs, spinal column, etc. We most commonly see them involving the radius and ulna in the upper extremity but
osteochondromas of the humerus and scapula are also common.
The growths in
multiple hereditary exostoses are not present at birth but almost all patients develop them before puberty. Once skeletal growth is done (mid- teenage years, several years after puberty), new
osteochondromas usually do not appear. There have been two genes associated with
multiple hereditary exostoses, EXT1 and EXT2. Almost all patients develop
multiple hereditary exostoses because they inherited it through one of these genes. The genes are autosomal dominant so there is a 50% chance a child will inherit this disorder if one parent has it.
The
exostoses (or
osteochondromas) can often be ignored but surgery is considered in a few situations. The first reason to think about surgery is pain. If painful, most commonly it hurts when the
osteochondroma is hit but also if it simply grows large enough to irritate nearby anatomical structures such as nerves. The second reason to consider surgery is if the growth of the mass is affecting other structures nearby. Again, this can be nerves or vessels but most commonly it is another bone. If an
osteochondroma grows on the undersurface of the scapula, it can rub against the ribs and be irritating. Body segments with two bones (radius and ulna in the arm and tibia and fibula in the leg) are at risk for problems with multiple
osteochondromatosis as the
osteochondroma can affect the growth of one of the bones. If the radius and ulna (the forearm bones) are not nearly the same length, movement will be affected (rotation of the forearm). O
steochondromas can slow down the growth of one bone or cause one bone to grow in an angled fashion. In either case, the balanced forearm can be thrown off kilter and problems can develop. Classically, the ulna near the wrist may be affected by an
osteochondroma, its growth slowed, and the radius continues to grow normally. Eventually, problems developed due to the mismatched length.
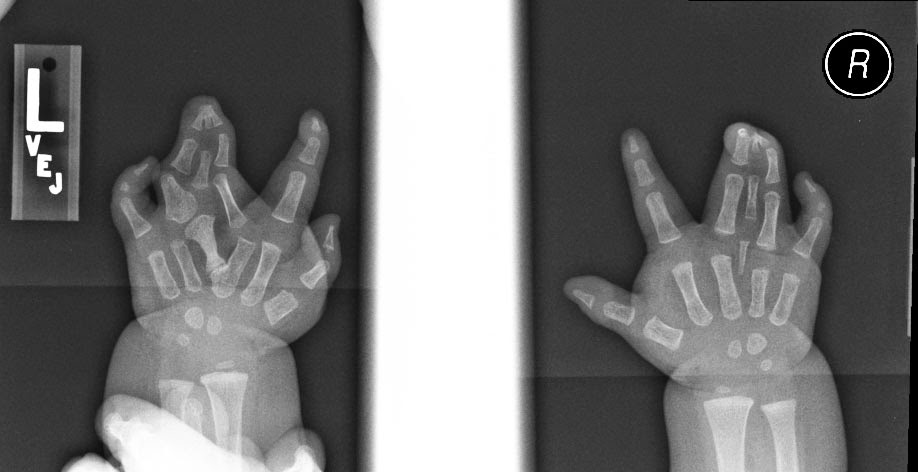
Here is one example. Both forearms have
osteochondromas affecting the distal ulna (near wrist) and the ulna has not grown as it should. The radius is therefore too long. On the left side, the radial head has dislocated at the elbow. On the right side, the radial head is in place but at risk.
![]() |
| Left arm from the back. Not the prominence of the dislocated radial head. |
![]() |
| Right arm from the back. The radial head is in place. |
![]() |
| Both elbows from the back. The left one is abnormal with a dislocation radial head. |
![]() |
| Left forearm. The radial head is out of position. See the osteochondroma on the distal ulna. |
![]() |
| In this arm, the patient has an osteochondroma on the distal ulna but the radial head at the elbow is still in place. |
We treated this patient to attempt to prevent the radial head on the right arm from dislocating. We sought to do this with an external fixator to lengthen the ulna bone.
![]() |
| External fixator to lengthen ulna to better balance the forearm. Slow growth of the ulna eventually achieves the appropriate length. |












.jpg)