When we consider congenital abnormalities of the upper extremity, most commonly, we think of extra bones or missing digits. However, there are many other conditions which fall under this umbrella and, therefore, the care of the congenital hand surgeon. The OMT classification (Oberg, Manske, Tonkin) has recently replaced the Swanson classification as the official classification scheme for birth anomalies of the upper extremity by the IFSSH. Section III is for Dysplasias or disordered growth and includes hypertrophy, see previous post on
macrodactyly and tumorous conditions. Vascular conditions including
hemangiomas and
malformations are thus classified.
Vascular lesions are either tumors or
malformations.
Hemangiomas are the most common blood vessel tumor and they are benign (i.e, not bad). Some consider these lesions a type of birthmark.
Hemangiomas are one of the most common tumors of early life. These tumors are either visible at birth (congenital) or present in the first weeks or months of life (infantile). The infantile
hemangiomas grow rapidly in the first 6 months to a year of life and then involute slowly (i.e., resolve). 50% have involuted by age 5, 70% by age 7 and most of the rest by age 13. There can be some
hemangiomas that are visible thereafter. The congenital
hemangiomas behave a bit differently as they are fully developed at birth and either disappear in the first year of life or persist.
There are different types of
hemangiomas including capillary, the most common in the upper extremity in my experience. These capillary
hemangiomas vary in appearance but one common type is the port- wine stain. The appearance is affected by the depth of the lesion. Superficial lesions look red and slightly deeper lesions maybe bluish.
Wikipedia has a good summary. Here is one capillary
hemangioma from Wikipedia.
![]() |
| Capillary hemangioma |
Other great pictures are visible online and one good website with nice images is
hemangiomaeducationThe bottom line is that most
hemangiomas do not require surgical treatment as they resolve with time. However, large
hemangiomas can become an appearance and social issue and family- physician discussions may be helpful.
The other type of lesion is the
vascular malformations. These are more common than tumors (approximately 2:1) They are typically not visible at birth and they grow with the child to become visible or symptomatic later in life.
Malformations occur when the baby is in the womb but, again, continue to grow (often very slowly) after birth and grow in proportion to the growing child. They can be venous, lymphatic, arteriovenous, capillary, etc. Venous
malformations are most common.
These children may become symptomatic anytime but typically present between ages 2-5. However, I also see such children for the first time in the teenage years. Typically, neither the patient nor the family knows when the malformation appeared and it becomes progressively more bothersome as it gets larger.
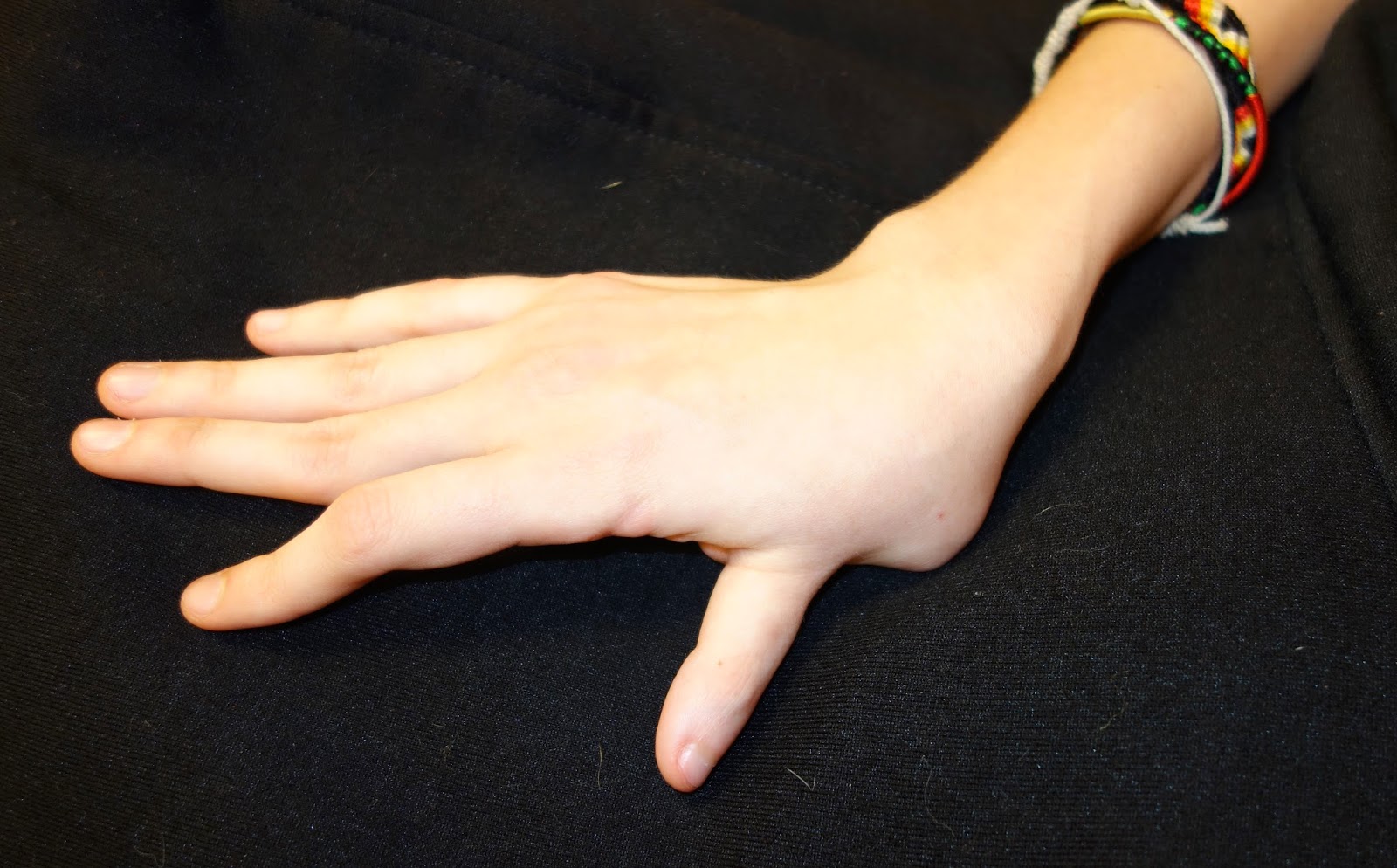
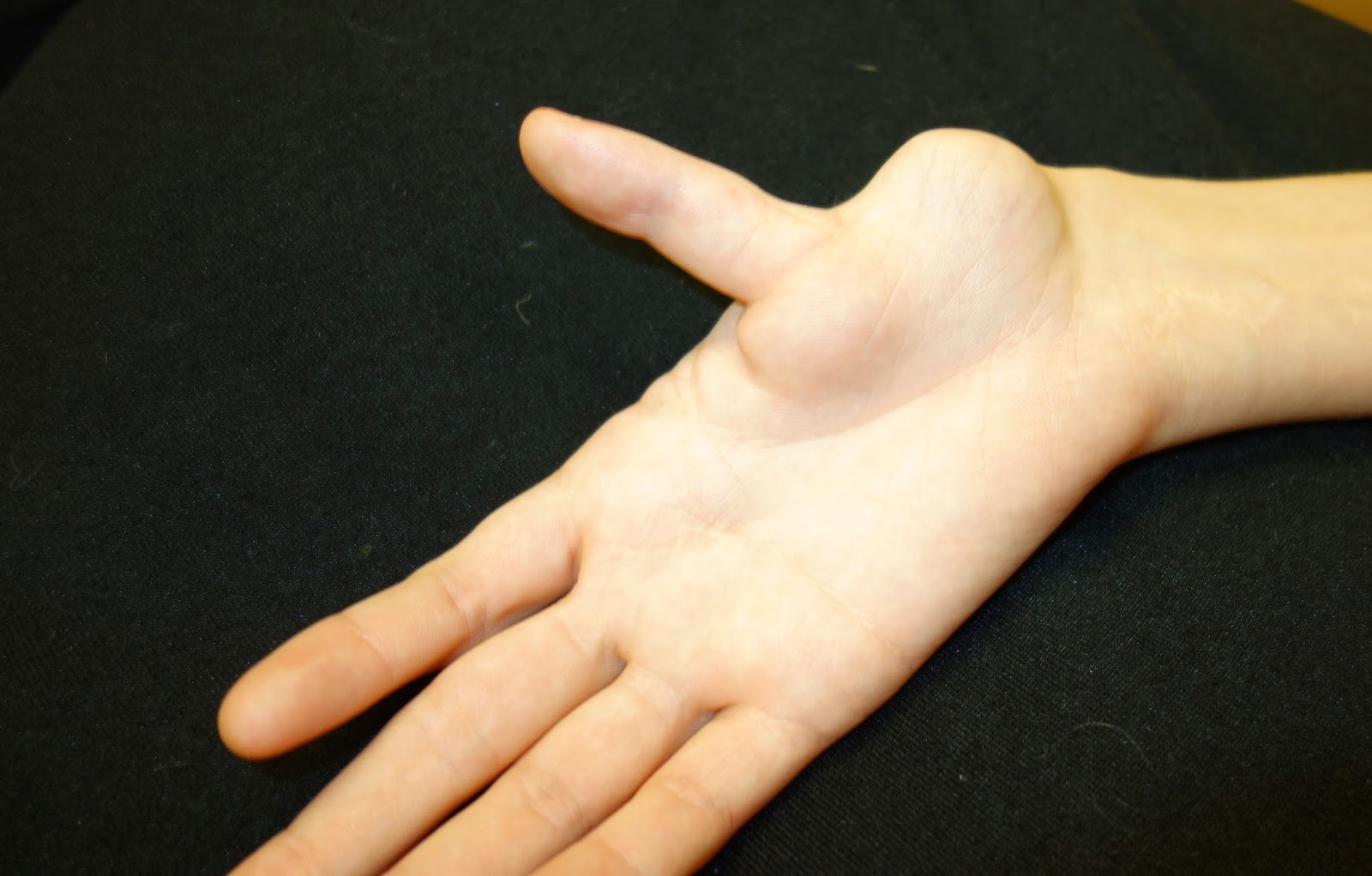
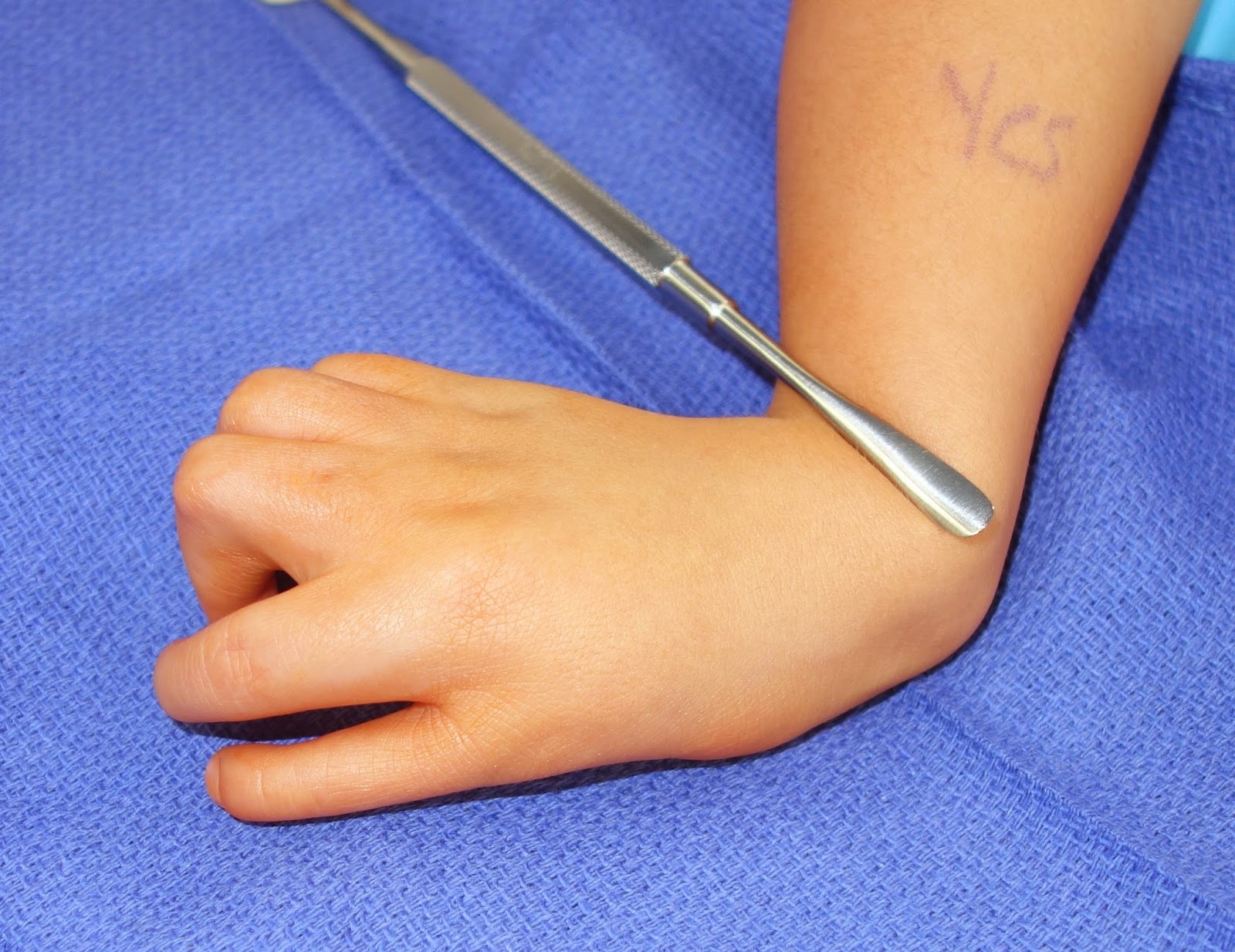
Here is one example with clinical pictures of a 15 year old male with pain and an enlarging mass in the finger. It is bluish sometimes and normal colored other times. It can increase and decrease in size. This picture is, in my experience, a common situation in that the lesion does not look that "bad." But, it is growing and can be painful. This patient and family requested surgical excision.
![]() |
| Venous malformation, ring finger over middle phalanx. |







































































.JPG)